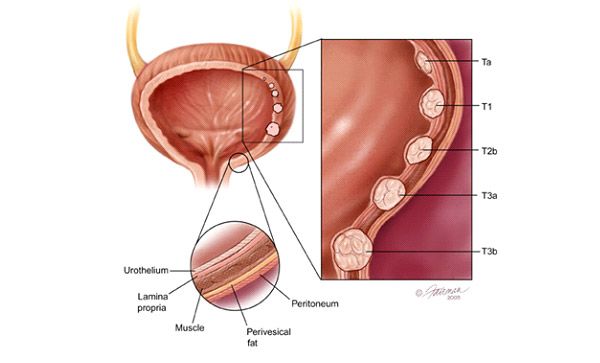
Figure 1: Staging of bladder cancer, based on the depth of invasion into the muscular wall of the bladder.
Most bladder cancers are detected early and confined to the epithelial lining of the bladder (stage pT1). Endoscopic removal of these tumours alone is curative (Figure 2) and all that is required is regular surveillance with cystoscopy to detect any recurrence.
However, bladder cancers that have invaded the muscular wall of the bladder (stage pT2-T4) are more aggressive and without definitive surgical treatment. At this stage, cancer will quickly spread to the lymphatic system outside the bladder and to distant organs. Once the bladder cancer cells have invaded the muscular wall, the only effective cure lies in radically removing the whole bladder and its surrounding lymph nodes and diverting the urine out of the body through either an artificial conduit using a loop of intestine or fashioning a new pouch from the intestine (known as a neobladder).
Agreeing to proceed with the surgery is a difficult decision for patients with muscle-invasive bladder cancer as they cannot accept the loss of their natural urination function and the need for a permanent pouch for the urine to leave the body. Many MIBC patients go into denial when faced with this diagnosis and do not follow up with their doctors, resulting in loss of valuable time and the opportunity for curative surgery.

Figure 2: Reconstruction of the urinary tract on multi-phasic computer tomography to visualize the kidneys, ureters and bladder.

Dr Tan Yau Min, Gerald
Dr Tan is a specialist urologist at Mt Elizabeth Hospital with over 17 years of clinical experience. He is internationally renowned for his expertise in minimally invasive and robotic surgery for prostate, kidney and bladder diseases. Dr Tan was one of the first surgeons to pioneer robotic nephron-sparing surgery in Asia, having performed the largest number of such surgeries in Mt Elizabeth Novena and Tan Tock Seng Hospitals to date. He was named the Outstanding Young Urologist of Asia by the Urological Associations of Asia in 2012.