A groin hernia refers to the protrusion of abdominal contents such as fat, small or large intestine through an area of weakness in the lower abdominal wall. These contents are wrapped in the inner lining of the abdominal cavity to form a balloon-like sac (Fig. 1).
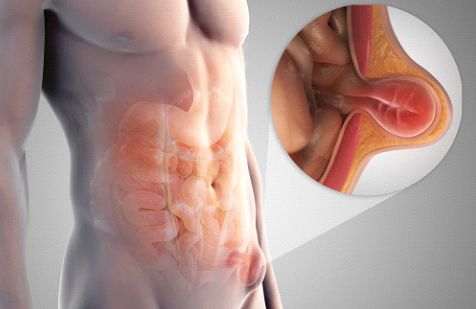
Figure 1: Illustration of a hernia, where abdominal contents protrude through an area of weakness in the abdominal muscle wall.
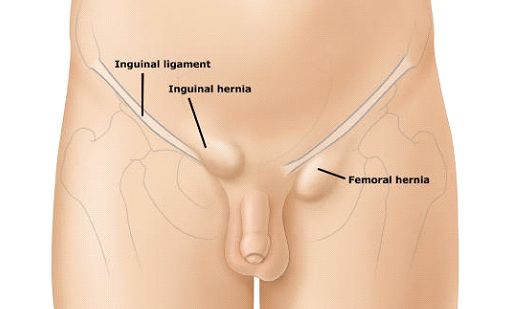
The majority of lumps in the groin are inguinal hernias (Fig 2). Less common causes of groin lumps are (1) femoral hernias; (2) swollen lymph nodes; (3) cysts or fatty lumps called lipomas of the spermatic cord; and rarely (4) swollen veins known as saphena varix. To identify which is the most likely cause for your groin lump, your doctor will usually ask you to lie down and cough a few times to see if and where the lump bulges out, and repeat the same manoeuvre with you standing upright. For greater accuracy, he may order an ultrasound of the groin to better visualize the anatomical location and contents of the lump.
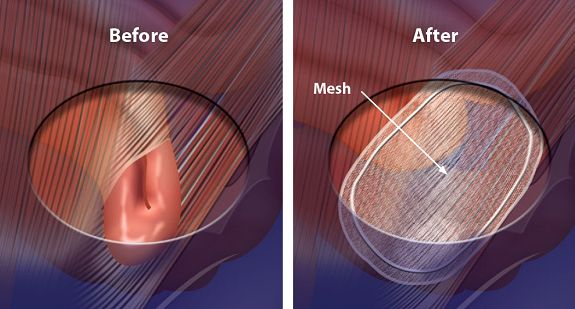
Surgeons performing surgical repair of inguinal hernias follow time-tested principles (Figs.3,4):
- Clear identification of the hernia sac or areas of defect in the muscle wall
- Reduction of the hernia sac and its contents back into the abdominal cavity
- Definitive repair of the abdominal wall using sutures and/or meshes
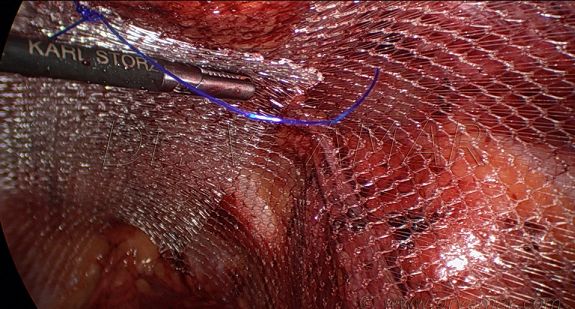
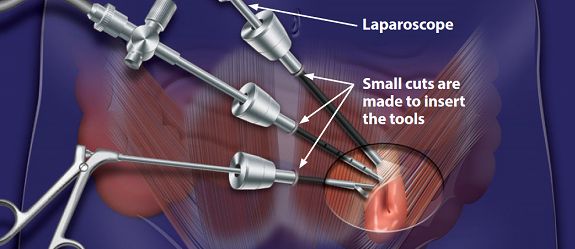
Repair of inguinal hernias may be performed using a conventional groin incision, or laparoscopically through small keyhole incisions <1cm. Most patients return home on the day of surgery, and the sensation of soreness over the wound usually resolves after 1-2 weeks after surgery. In 90-95% of patients undergoing hernia surgery, the repair is successful and the hernia does not recur.
Minimally invasive (laparoscopic) surgery has several advantages over conventional surgery – the incisions are small and look nicer; patients have less pain and quicker recovery after surgery; and are able to return to work and regular activities much sooner (Fig. 5) . However, laparoscopic surgery costs slightly more than conventional open surgical repair, and in some cases may not be feasible or be the most appropriate approach. Some of these scenarios include (1) painful incarcerated or strangulated hernias; (2) large hernias extending into the scrotum; (3) patients being morbidly obese; and (4) patients not being able to tolerate general anaesthesia. In such scenarios, open surgical repair still gives the best clinical outcomes.