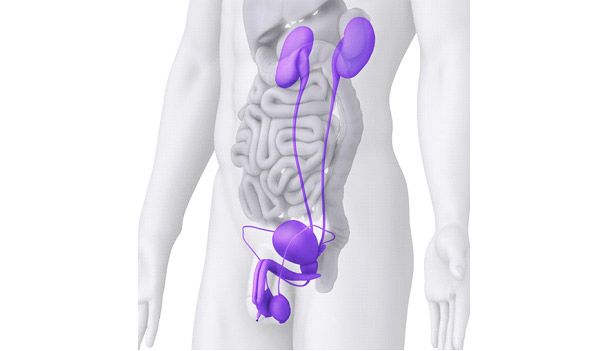
Urine is produced by the two kidneys situated in the abdominal cavity. It is excreted down long narrow tubes called the ureters into the bladder. When the bladder is full, urine is passed out through the prostate and urethra in men (in women, the prostate is absent) (Fig. 2).
In Singapore, the three commonest causes of blood in the urine are infections, stones, and cancers or growths of the kidneys, ureters, bladder or prostate. Less common causes of haematuria include (1) trauma/ injury to the urinary tract; (2) kidney diseases such as autoimmune nephropathy and glomerulonephritis; (3) benign familial haematuria; and (4) sickle cell trait. Your general practitioner is likely to refer you to a urologist for further evaluation of blood in the urine.
A CT urography scan with intravenous contrast takes about 10-15 minutes to complete, and is performed in the Radiology Department. After a preliminary scan of the abdomen and pelvis without contrast (to look for urinary stones), the radiology technician will inject intravenous low-dose iodinated contrast through a small intravenous cannula in the dorsum of the hand. The scan is then repeated 2 and 10 minutes later to assess for any abnormalities in excretion of contrast down the urinary tract, and to look for enhancing lesions such as tumours or cancers. Multi-phasic CT urography is the imaging procedure of choice because it has the highest sensitivity and specificity for imaging the upper tracts1 (Fig 3).

In patients with existing kidney impairment, the intravenous contrast poses a small risk of causing further damage to the kidneys. Nowadays, this risk is mitigated by using low-dose iodine contrast together with agents like N-acetylcysteine2. In patients with contrast allergy, magnetic resonance urography is an acceptable alternative imaging approach.