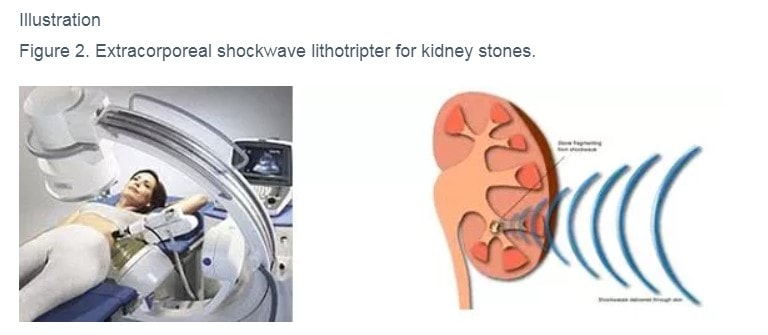
ESWL is a popular treatment for stones <2cm in size in the kidneys and upper ureter. It is performed as an outpatient procedure and involves the patient lying on a specially constructed treatment platform. Shock waves of varying intensities are created outside the body and transmitted through the skin and body tissues to converge on these stones. The stones are then shattered into smaller particles that pass easily through the urinary tract in the urine (figure 2). Recovery time is relatively short, and most people can resume normal activities in a few days. Side effects of ESWL treatment include bruising and pain around the treated kidney; downstream blockage of stone fragments in the lower ureter; and incomplete stone clearance requiring multiple treatment sessions.
For stones in the lower ureter <2cm, specially constructed small-calibre endoscopes are passed up the ureter to the stone’s location with the aid of guide-wires under X-ray guidance. The stones may then be shattered using a laser probe under direct vision, and the fragments retrieved out of the ureter using special stone baskets. If the ureter or kidney is swollen from stone obstruction, a temporary plastic stent is left in the ureter to facilitate healing and is subsequently removed using a cystoscope 2-4 weeks after the initial procedure. URS is usually performed as an outpatient procedure under general anaesthesia. Pain after URS usually resolves after 2-3 days, although blood in the urine will take slightly longer to clear up.
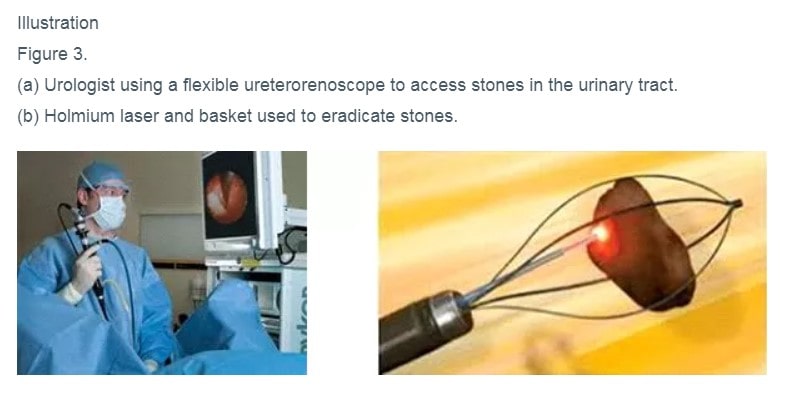
In recent years, advances in endoscope technology have enabled urologists to use small-calibre flexible ureterorenoscopes to steer all the way up the upper ureter into the kidney, and remove kidney stones using lasers and stone baskets (figure 3). This has proved most successful for definitive clearance of stones located in the lower chambers of the kidney and larger stones above 1cm in size, for which ESWL has poor stone clearance rates.
For kidney stones > 2cm in size or occupying a significant part of the kidney (known as staghorn stones), PCNL is the treatment of choice for definitive stone clearance. Depending on the anatomy of the kidney or stones, sometimes this can also be the optimal procedure for stones 1cm and larger in size.
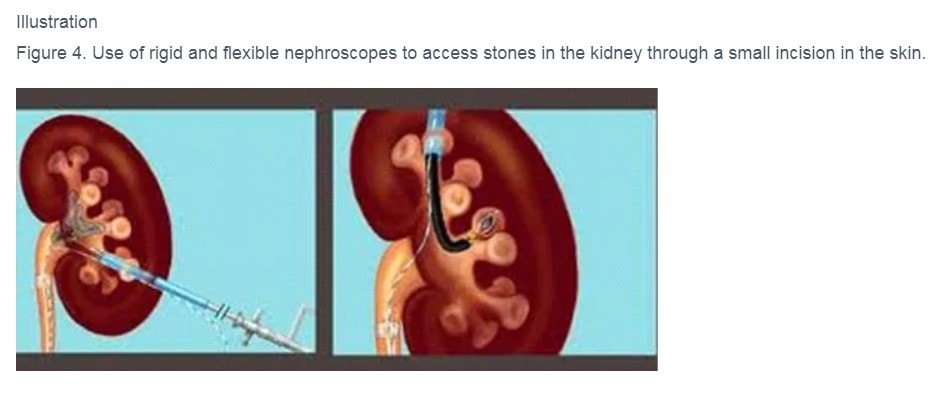
This procedure is performed under general anaesthesia.With advances in surgical technique, it can be performed usually with the patient lying supine on the surgical table. Under X-ray or ultrasound guidance, the urologist makes a tiny incision in the back and creates a tunnel directly into the relevant chamber of the kidney. Rigid and flexible nephroscopes are used to locate to the stones, which are then shattered and removed using various devices (figure 4). An internal ureteric stent is usually placed at the end of the procedure to allow for healing, usually for 1-2 weeks. Newer technology, equipment, and surgical techniques allow for smaller endoscopes to be used, with smaller incisions and lower risk of complications such as bleeding and pain. This is known as mini PCNL. Most patients can be discharged on the same day (day surgery) or after an overnight stay of 1 night.
Comparing mini PCNL to ureterorenoscopy for stones larger than 1cm located in the lower part of the kidney, mini PCNL was found to have a higher stone-free rate