In patients with obstruction at the junction between the kidney pelvis and the ureter (known as ureteropelvic junction obstruction or UPJO), the blocked kidney becomes swollen, causing patients to experience persistent loin pain or ache (Fig.1). If the blocked kidney becomes infected, there may be associated fever, chills, painful urination and passage of bloody urine. When these symptoms are persistently ignored, the swollen kidney will start to deteriorate and irreversibly lose its function when the nephrons are replaced by scar tissue (interstitial fibrosis).
UPJO affects 1 in 1,500 people, and occurs anytime from birth to old age1. In adults, it usually arises from kidney stones, fibro-epithelial polyps or previous kidney surgery. It may also arise when the crossing vessels supplying the lower portion of the kidney compress on the ureter-kidney pelvis junction.
Fig 1. The kidneys produce urine which is carried down the ureter into the bladder. In ureteropelvic junction obstruction, urine outflow is impaired and the kidney becomes swollen.

UPJO may be suspected when patients present with persistent loin or upper abdominal pain. Ultrasonography of the affected kidney will usually reveal significant hydronephrosis, sometimes with associated kidney stones. Definitive diagnosis is usually made on high-resolution contrast-enhanced computer tomography (CT) scan of the abdomen, which is both highly sensitive and specific. In patients with renal impairment, MRI kidneys with 3-dimensional reconstruction is an alternative imaging modality that allows precise visualization of the anatomy and blood supply of the obstructed ureter-pelvic junction (Fig. 2).
Fig.2 CT 3-dimensional reconstruction of the vessels supplying both kidneys.
However, not all kidneys that appear swollen are truly obstructed. It is therefore essential to perform diuretic nuclear renography to confirm the presence of functional obstruction and the differential function of the two kidneys. In this regard, the 99mTc-MAG3 (mercaptoacetyltrigycine) scan is the preferred investigation of choice. Clearance of half the isotope from the affected renal pelvis which takes more than 20 minutes is confirmatory of functional obstruction.
In patients with UPJO confirmed on both CT/MR imaging and diuretic renography demonstrating impaired excretory function of the affected kidney, surgery should be performed to relieve the obstructed kidney and restore kidney function. There are a variety of surgical approaches to relieve the obstructed ureter-pelvic junction.
Pyeloplasty via a large abdominal incision has been the traditional surgical approach for repairing UPJO. The Anderson-Hynes dismembered pyeloplasty remains the most popular approach, where the narrowed segment is removed and the remaining healthy tissue from pelvis and ureter are reattached with sutures (Fig.3) over an internal silastic ureteric stent. Once the sutures have healed, the ureteric stent is then removed from the bladder using a cystoscope a few weeks later. In patients whose kidney pelvis is large and redundant, or who have a long length of narrowed proximal ureter, a spiral flap repair (Culp-De Weerd non-dismembered pyeloplasty) may be a more appropriate approach (Fig 4).
Fig 3. Anderson-Hynes dismembered pyeloplasty

Fig. 4. Spiral Culp-De Weerd non-dismembered pyeloplasty for patients with a long segment of narrowed proximal ureter.

Endopyelotomy is an alternative approach to relieving UPJO. In antegrade percutaneous endopyelotomy, a needle tract is made through the flank muscles into the swollen kidney pelvis under X-ray guidance, which is then dilated to permit passage of a rigid nephroscope into the kidney. The nephroscope is then used to make a full-thickness incision across the narrowed segment using a sharp blade under direct vision, and a ureteric stent is left to permit healing of the ureter-pelvic junction (Fig.5). Alternatively, the narrowed segment may be incised from a retrograde approach using a Holmium laser passed through a narrow ureteroscope, although the recurrence rate is higher for the latter approach.
Success rates for published series of endopyelotomy surgeries (74-95%) are not as good as those reported for pyeloplasty (>90%). In recent years, the superior long-term results reported with laparoscopic and robotic pyeloplasty have led to endopyelotomy falling out of favour with urologists. Endopyelotomy is also not recommended for patients with narrowed segments >2cm, kidney function <25%, and presence of severe hydronephrosis.
Fig. 5. Antegrade percutaneous endopyelotomy, where a cold-knife is used to make a full-thickness incision across the narrowed ureter.

Yes! In the past decade, minimally invasive surgery techniques which replicate the surgical principles of open pyeloplasty have become very popular. The same surgery to relieve UPJO may now be safely performed with laparoscopic instruments or using the da Vinci® surgical robot (Intuitive Surgical, Sunnyvale, USA) through small incisions in the abdomen. Laparoscopic or robotic pyeloplasty affords numerous advantages over conventional open kidney surgery – patients have less pain and intraoperative bleeding, shorter hospitalization stay, earlier return to work and normal activities. For open surgery, many patients complain of chronic pain or numbness over the large incision (Fig. 6).
Fig. 6. A. Patient with traditional abdominal flank incision for open pyeloplasty. B. Keyhole incisions <1.5cm used during laparoscopic or robotic pyeloplasty.

Robotic surgery refers to the use of a robotic surgical platform known as the da Vinci® Surgical System (Intuitive Surgical, Sunnyvale, USA) to perform minimally invasive surgery through small incisions. This innovative technology comprises a surgical cart that is docked next to the operating table to small ports placed through incisions >1cm in the patient’s abdomen. Robotic wristed instruments are then passed through these small ports into the abdomen, which are controlled by the surgeon sitting at the operating console some distance away from the operating table. A binocular camera lens affords the surgeon a 3-dimensional view of the operating field, which can be magnified up to 12 times. The surgeon then manipulates the camera lens and the various robotic instruments at the console using the hand controls and pedals. These specially designed wristed instruments afford the surgeon excellent precision and dexterity of surgical movement (Fig.7). Recent published data strongly suggests that robotic pyeloplasty delivers superior results to laparoscopic pyeloplasty and endopyelotomy – this is likely due to better tissue handling and improved surgical dexterity afforded by the robotic instruments. Robotic pyeloplasty is especially appropriate for patients with previously failed surgeries that now require secondary UPJO repair, where precision and delicate handling of the local tissues is crucial for operative success2-4.
Fig. 7: The da Vinci® Surgical System comprises a patient cart docked next to the patient on the operating table, while the surgeon operates from a console.

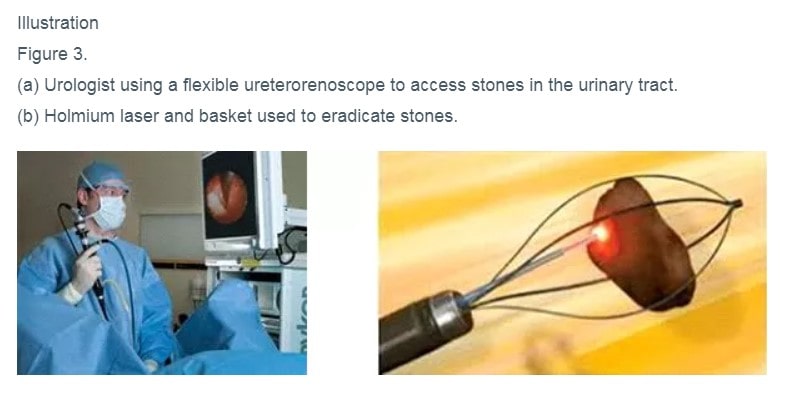
In recent years, advances in endoscope technology have enabled urologists to use small-calibre flexible ureterorenoscopes to steer all the way up the upper ureter into the kidney, and remove kidney stones using Holmium lasers and stone baskets (figure 3). This has proved most successful for definitive clearance of stones located in the lower chambers of the kidney, for which ESWL has poor stone clearance rates.
In kidneys that become obstructed due to stones impacted in the ureter or the ureter-pelvis junction, a variety of techniques are available to clear the obstructing stone(s). These include (1) percutaneous nephrolithotomy, where a rigid scope is passed into the kidney via a tract through the flank muscles and the stones blasted using ultrasonic or pneumatic energy; (2) extracorporeal shockwave lithotripsy, where the stones are targeted and fragmented under X-ray guidance using a high-energy shockwave machine; or (3) retrograde laser lithotripsy, where a slender ureteroscope is passed through the bladder up the ureter to the level of the obstructing stone and a Holmium laser fibre used to fragment the stone(s) (Fig.8).
Fig 8. Illustration of a ureteroscope being advanced up the ureter to the obstructing stone, which is then fragmented using a laser fibre.

In cases of kidney obstruction due to tumours in the ureter (known as transitional cell cancer), treatment is based on the aggressiveness of the local tumour. In cases of early cancer growth, these may be ablated using the Holmium laser energy administered via the ureteroscope. In more advanced cases where these upper tract cancers have become locally invasive, the entire length of the affected ureter and kidney must be removed to prevent cancer recurrence or progression. Nowadays, the latter procedure (known as radical nephroureterectomy) is routinely performed using laparoscopic or robotic instruments as well.