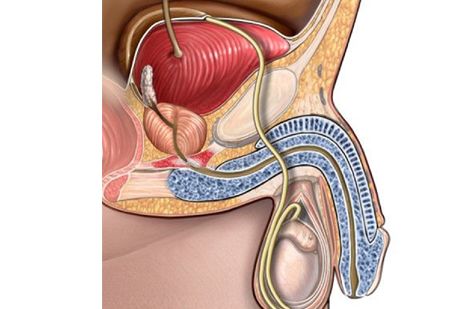
The prostate is a walnut-sized gland that is part of the male reproductive system and is found below the bladder in the deepest part of the male pelvis (Fig.1). The prostate gland helps produce and store seminal fluid, which is an important component of semen that helps provide nourishment for sperm. It wraps around the urethra below the bladder outlet, and together with the pelvic floor muscles is involved in the control of urination.
The risk of developing prostate enlargement in Singapore increases with age because as men get older, their prostate glands will invariably enlarge in size. This can result in one or more possible problems: (1) mechanical obstruction of the prostatic urethra and bladder outlet, leading to slow urinary stream, difficulty starting urination, and incomplete bladder emptying; (2) inflammation of the prostate (known as prostatitis), where patients may experience urgent and frequent urination, pelvic discomfort or blood in the urine; and (3) cancerous change within the prostate gland, which if undetected may gradually then spread outside the prostate to the nearby lymph nodes and thereafter the bony skeleton.
Treatments for prostate enlargement in Singapore include prescription medication, minor procedures and surgeries. One common prostate enlargement treatment in Singapore includes medication. For most patients, medication like alpha-blockers works effectively to relax the prostate and eases the flow of the urinary stream. However, surgery is another viable treatment option to manage an enlarged prostate in Singapore. Most urologists will recommend the surgical route if patients do not respond to the medication. Surgical methods include Transurethral resection of the prostate (TURP) and GreenLight™ Laser system, which are some examples of prostate enlargement treatments in Singapore.
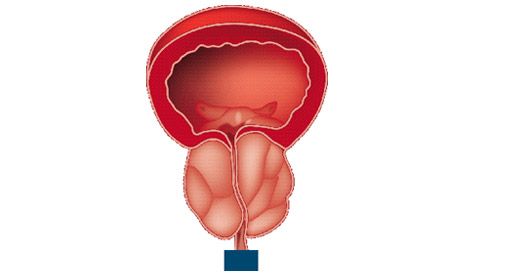
In men above the age of fifty, progressive enlargement (hyperplasia) of the prostate gland often causes a mechanical blockage to the prostatic channel and bladder outlet. This results in symptoms of difficulty starting urination, a slow urinary stream, and a sensation of incomplete bladder emptying. If left ignored for a long period of time, patients are likely to develop the inability to pass urine (acute urinary retention), bladder stones, recurrent urinary tract infections, and eventually obstructive kidney damage.
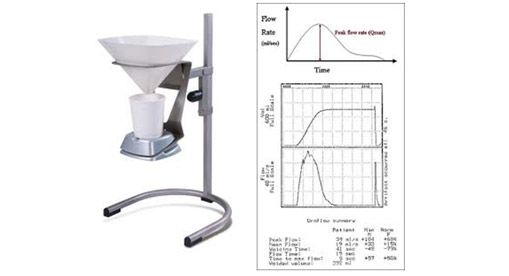
Once patients notice these symptoms, they should consult their urologist, who will usually perform the following investigations to assess the cause and extent of their urinary obstruction: (1) bedside ultrasonography of the prostate, bladder, and kidneys; (2) uroflowmetry and residual urine measurement (Fig. 2); (3) digital rectal examination of the prostate to palpate for possible nodules on the prostate; and (4) blood tests to assess kidney function and the likelihood of prostate cancer (known as prostatic-specific antigen or PSA).
In younger men with similar symptoms and a normal-sized prostate, or in chronic smokers with associated blood in the urine, the urologist may recommend further evaluation with cystoscopy, where a flexible endoscope is passed up the male urethra to assess the lower urinary tract for urethral strictures or bladder tumors as alternative causes for such obstructive symptoms.
For most patients with early prostate obstruction, their symptoms are usually well controlled with medications known as alpha-blockers, which act on receptors in the bladder neck to relax the bladder outlet during urination. For men with large prostate glands more than 40gm in size, combination therapy of alpha-blockers with 5α-reductase inhibitors (5ARIs) e.g. finasteride, has been demonstrated in several large studies to improve urine flow rates, and bladder emptying, as well as to reduce the likelihood of developing episodes of urinary retention. The latter acts by inhibiting the growth of cells within the prostate, and when taken over a prolonged period, it will help decrease prostate size. However, 5ARIs are often associated with erectile dysfunction and loss of libido, as they also interfere with the effects of testosterone on the rest of the body. More recently, daily low-dose Cialis® (tadalafil) has also been reported to improve urinary flow and may be considered as an alternative treatment to alpha-blockers in men with both prostate obstruction and erectile dysfunction.
In patients whose obstructive prostate symptoms are not improving with medications, most urologists will recommend a type of prostate enlargement treatment in Singapore known as transurethral resection of the prostate (TURP) as the next treatment option. In TURP, once the patient is anesthetized, the urologist passes a specially designed rigid endoscope up the penile urethra to reach the prostate gland. A cutting loop with a high-energy electrical current is used to widen the prostatic channel by shaving away prostate pieces, which are then evacuated from the bladder by a special handheld pump and sent for laboratory assessment. After the prostatic channel is adequately widened, a urinary catheter is inserted through the urethra into the bladder, and irrigation is commenced to wash out any bleeding from the raw surfaces of the prostate gland. This is usually stopped the following day, and the catheter is removed 2-3 days after TURP surgery. In most cases, patients have significantly improved urine flow and are discharged without complications.
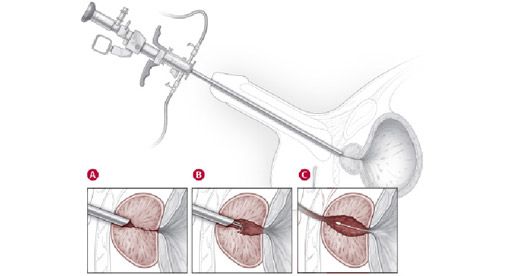 Fig 4. Illustration of transurethral resection of the prostate, where a high-energy cutting loop is used to serially cut prostate chips from within to widen the prostatic channel.
Fig 4. Illustration of transurethral resection of the prostate, where a high-energy cutting loop is used to serially cut prostate chips from within to widen the prostatic channel.
The main risk of TURP surgery is persistent significant bleeding from the cut surfaces of the prostate gland, which occurs in 5% of all cases. If present, it may cause clot retention of the bladder, where urine is not able to drain out of the blocked catheter. This will necessitate blood transfusion, and manual washout of the clots through the catheter, and if unsuccessful, patients will need to return to the operating theatre for washout of the clots under anesthesia. This risk is higher in patients with acute urinary retention; those with very large inflamed prostate glands; and in patients on anticoagulants e.g. aspirin, warfarin, Plavix®, etc. Less common complications include bladder perforation, temporary urinary incontinence, or delayed scarring of the bladder neck or urethra with a recurrence of obstructive urinary symptoms.
Compared to earlier TURP technology using monopolar electrical energy, the incidence of such complications has dropped significantly with the advent of bipolar TURP2. In bipolar TURP, the high energy cutting loop allows the surgeon to cut and stop bleeding simultaneously, with much less collateral energy damage to the nerves in the pelvic floor and urinary sphincter. In addition, the use of normal saline as irrigation fluid in bipolar TURP (instead of glycine) has minimized the risk of TUR syndrome. This means that urologists are no longer under time pressure to stop the surgery after an hour for fear of causing the patient to become fluid overloaded with electrolyte imbalances and can complete the surgery successfully in one sitting regardless of prostate gland size. As such, bipolar TURP devices have replaced monopolar TURP in most hospitals today as the standard operating system and are recommended by the European Association of Urology for improved clinical outcomes.
The Greenlight™ Laser is an innovative laser system that uses either a kalium-titanyl-phosphate (KTP) or a lithium triborate (LTO) laser at 532nm wavelength to widen the prostatic channel by vaporising the prostate gland at high energy. The laser energy is absorbed by haemoglobin instead of water, resulting in immediate ablation of prostate tissue with minimal bleeding during the procedure. The benefits of GreenLight laser vaporization of the prostate for patients with prostate enlargement in Singapore include a shorter hospital stay and catheter time, and less intraoperative bleeding. However, as the prostate tissue is vaporized, no tissue is available for laboratory analysis for the presence of cancer cells in the prostate.
In 2015, three different GreenLight™ lasers were in clinical use – the 80-W (KTP), 120-W HPS (LTO), and 180-W XPS (LTO) lasers. The latter two laser systems (American Medical Systems, Minnetonka, USA) are currently in use in Singapore, with the 180-W XPS swiftly gaining popularity. The intermediate-term functional results of 532nm GreenLight™ laser vaporization therapy are comparable to TURP surgery3. There are also several papers validating its safety in “difficult prostates” such as patients with large glands >80ml, on anticoagulants, and those in urinary retention4. Given the published scientific data, the European Association of Urology now recommends GreenLight™ laser therapy as a safer surgical alternative to TURP surgery and if available, should be considered as first-line treatment in patients on anticoagulants or at high cardiovascular risk.
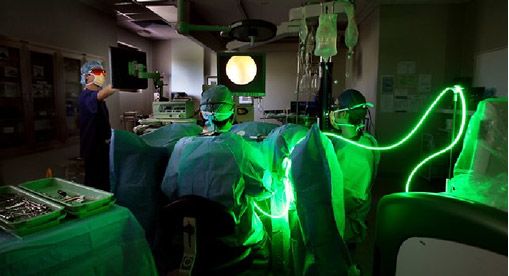 Fig 5. Urologist performing GreenLight™ laser vaporization of the prostate.
Fig 5. Urologist performing GreenLight™ laser vaporization of the prostate.
Robotic surgery refers to the use of a robotic surgical platform known as the da Vinci® Surgical System (Intuitive Surgical, Sunnyvale, USA) to perform minimally invasive surgery through small incisions. This innovative technology comprises a surgical cart that is docked next to the operating table to small ports placed through incisions < 1cm in the patient’s abdomen. Robotic wristed instruments are then passed through these small ports into the abdomen, which are controlled by the surgeon sitting at the operating console some distance away from the operating table. A binocular camera lens affords the surgeon a 3-dimensional view of the operating field, which can be magnified up to 12 times. The surgeon then manipulates the camera lens and the various robotic instruments at the console using hand controls and pedals. These specially designed instruments afford surgeons excellent precision and dexterity in surgical movement because of their patented robotic wrist technology.
 Fig. 6: The da Vinci® Surgical System comprises a patient cart docked next to the patient on the operating table, while the surgeon operates from a console some distance away
Fig. 6: The da Vinci® Surgical System comprises a patient cart docked next to the patient on the operating table, while the surgeon operates from a console some distance away
In Singapore and the United States today, 90% of all surgeries to remove the entire gland in prostate cancer are now performed using the da Vinci robot. However, its use for benign prostatic obstruction has been fairly limited to patients with very large prostates > 100ml, where open simple prostatectomy had previously been the standard treatment approach5. In robotic-assisted simple prostatectomy, the centrally enlarged portion of the prostate gland is surgically removed by making an incision in the bladder through small incisions in the abdomen. The high cost of this procedure and prolonged catheter time required for the bladder incision to heal, makes this novel approach unlikely to become popular with patients when other prostate enlargement treatments in Singapore described above are now able to deliver superior clinical outcomes at a lower cost.